Posted by Melinda Monge on Wednesday, January 9, 2019
Author: Carmenisha Ward
My collaborative research efforts this summer taught me that social determinants play a huge role in the quality of healthcare that an individual receives. A person’s neighborhood,income, education, skin color and even sexual orientation determines the type of medical attention that person can access. Social determinants also influence which people have a higher probability of contracting certain illnesses. If a person happens to have the “wrong”skin color or the “wrong” income, he or she has a higher probability of having limited access to resources that are readily available to those with all the “right” social attributes. This situation is the definition of a disparity.
According to the CDC, the top candidate for HPV-related cancer is the MSM community.
What Disparity and Why?
The leading cause of all HPV-related cancers is, of course, HPV. So what is it and why is the MSM population so vulnerable?
● HPV, also known as human papillomavirus, describes a group of over 150 viruses. With over 14 million new infections each year, HPV is the most common sexually transmitted infection (STI) in the United States. Most of the HPV related incidences of cancer are caused by high-risk viruses type 16 and type 18.(1)
● HPV high-risk viruses are reported to be responsible for 2% of new cancer cases, which is over 30,000 incidences. The majority of these incidences will be MSM. (1)
● According to the CDC, HPV incidence rates are increasing in MSM compared to other cohorts, such as heterosexual men and women. (4)
● Research also reveals that although a significant portion of the MSM population has heard of HPV (74%), less than half know that the STI causes health problems for males and even fewer had knowledge about associated illnesses such as cancer. (3)
● A significant portion of the MSM population has HIV, which weakens the immune system. (1)
Eliminating the Disparity
There is strong indication that education is the biggest gap that creates the disparity for the MSM community. After being educated about HPV-related cancers, the following was said by members of the MSM community:
“I had no idea that it caused all of those cancers. I think if that was made public knowledge [people would get vaccinated]”
“knowing the facts is the most important part because once you know then you realize this shouldn’t be disregarded and there’s a vaccine you should probably get”.(2)
In order effectively reach the greatest number of people we have to work with community organizations. The MSM community prefers organizations that welcome and support their sense of identity. Places that already have an established relationship with MSM are the best places to implement an education program because they already know the population and how to best relay the necessary information. The MSM will also have the opportunity to come back to get more information if necessary. If this population can be empowered with knowledge, they will have the ability to make sure they can approach their healthcare provider to ask for the necessary preventive care.
Conclusion
There’s an old saying, “If you know better, you do better.” Information has to be given to as many people as possible in language that is easily understood by the people. As more community organizations begin to gain reputations as health literacy hubs, I believe that the MSM HPV-related cancer disparity will start to disappear.
References:
1. Centers for Disease Control and Prevention. (2017, April 26). Retrieved from https://www.cdc.gov/
2. Fontenot, H. B., Fantasia, H. C., & Zimet, G. D. (2017). Increasing HPV Vaccination and Eliminating Barriers: Recommendations From Young Men Who Have Sex With Men. Journal of Adolescent Health, 60(2). doi:10.1016/j.jadohealth.2016.10.424
3. Koskan, A. M., & Fernández-Pineda, M. (2018). Human Papillomavirus Vaccine Awareness Among HIV-Positive Gay and Bisexual Men: A Qualitative Study. LGBT Health, 5(2), 145-149. doi:10.1089/lgbt.2017.0109
4. Welbeck, M. (2016). Anal Pap Screening for HIV-infected Men Who Have Sex With Men: Practice Improvement. Journal of the Association of Nurses in AIDS Care, 27(1), 89-97. doi:10.1016/j.jana.2015.08.008
Disclaimer
The views expressed in this paper are exclusively those of the author and not necessarily representative of the organizations the author represents nor the ChicagoCHEC organization. This work is solely intended to help further disseminate information related to ChicagoCHEC’s cause and stimulate dialogue about important topics. It is not a report by ChicagoCHEC itself and must not be treated as such.
Posted by Melinda Monge on Wednesday, December 19, 2018
Commentary: Networking as a form of advocacy
Author Information: Estefania Perez-Luna, BS Health Science, Benedictine University, ChicagoCHEC Research Fellow.
Author Background: Estefania is an emerging bilingual health professional with experience with immigrant Spanish-speaking communities. She is a recent first generation college graduate from Benedictine University with a degree in Health Science and aspires to become a physician with a dedication towards marginalized communities of color.
Conflict-of-interest Disclosures: There are no conflicts of interest present.
Disclaimer: The views expressed in this paper are exclusively those of the author(s) and not necessarily representative of the organizations the authors represent nor the ChicagoCHEC organization. This work is solely intended to help further disseminate information related to ChicagoCHEC’s cause and stimulate dialogue about important topics. It is not a report by ChicagoCHEC itself and must not be treated as such
Several weeks into the ChicagoCHEC Fellows Program, I came to learn several important lessons. One particularly stands out to me as a first-generation rising health professional. That is the concept of mentoring and along with it networking and self-advocacy.
I never understood what people meant by “It’s not what you know, but who you know,” but I think now I understand the importance of this. And no, it does not mean that connections are all that matters, but it means that aside from your actual qualifications (“what you know”), it is the connections you make that will connect you to opportunities.
Being part of this Research Fellows Program has made me reflect more deeply on what the underserved communities face, as it relates to health disparities. I’ve learned how inequity through unequal power and unequal life opportunities in society impact the health and well-being of not only individuals but entire communities. However, I have also reflected on how this is also true at an individual level for first-generation students like myself.
As I alluded to earlier in the idea of unequal life opportunities, first-generation students have grown upwith social inequities. Social capital, the relationships and network that an individual uses, is one example of an unequal opportunity. Students from affluent and professional backgrounds are born with a wealth of social capital. Their families early on expose them to different careers and different opportunities. Perhaps their parents are doctors, their uncle a lawyer, or their aunt a researcher. This early exposure is crucial, as it gives them a wealth of information to consider and a world to explore which helps shape their career choices. By the time they get to college, they’ve already learned what college is and most likely have developed a wide variety of knowledge on the career choices they can make. Perhaps they’ve shadowed their parents at a hospital, or have heard countless stories from their uncle about what it is like to be a lawyer. They have had these people around them to provide advice and answer questions well before they reach college.
In contrast, someone like myself from an immigrant low-income family, was born into circumstances where that wealth of social capital has been missing. I, the daughter of a woman with a first grade education and the daughter of a man with a sixth grade education, could not turn to my parents or my family to find out what college was like, what being a doctor was like, or what being an engineer was like. When I first arrived to college, I did not even know what a bachelor’s degree was or what credit hours were. However, my parents did instill in me the importance of education and with that value in mind, I decided to pursue college despite barely understanding what college was about. Luckily, when I made it to college, I found myself with a few people who saw a potential in me and invested in me enough to give guidance and advice. I did not realize it at the time but I had been mentored. I continued to strive for academic excellence and with the support and guidance of others, I became the first person in my family to graduate from college.
During college, I did learn about the idea of mentorship but I did not have a full understanding of its importance. As I have participated in this program, I have become more informed on just how important that is and I wish I had come to this realization sooner. Listening to many healthcare professionals who come from similar backgrounds tell us about their journey into a health career, I have noticed a common pattern. They all emphasize the role that other people’s mentorship played in helping them succeed not only in college but throughout the rest of their lives in their careers. It is here I came to the realization that mentorship and networking are a crucial component to succeeding in a career. I understood that people from affluent backgrounds are born with a social network around them that is not only long term, but will also continue growing to serve as a vital resource in their career path.
In contrast, first generation students who are born lacking that social network, must work to fill in those gaps of by themselves. Because no one in our families can be that support and guide, we must instead seek it out on our own externally through mentors. A special emphasis should be noted on the word mentors not mentor, meaning that a network of people is essential to succ essfully navigate one’s career. Being part of the ChicagoCHEC Fellows Program, I have learned that in mentorship there is a wide spectrum in terms of types. Mentors can vary in terms of level of engagement, for example some mentors choose to take their mentees fully under their wing and follow them closely to provide ample support and guidance. Other mentors may make referrals to connect the mentee to other people or opportunities, these are called sponsors. Other mentors are less engaged and expect the men tee to approach them when necessary; they tend to provide quick advice and guidance. Additionally, mentors can vary in terms of function. Not one mentor has all the answers and knowledge on all areas, therefore, mentors can provide guidance based on specific areas of expertise. Depending on their experience, they can provide guidance on navigating college, the technicalities of a specific career, and even on creating a vision with purpose regardless of the career choice the mentee chooses. Rather than think ing of mentorship as being one person guiding someone, mentorship needs to be thought of as a comprehensive network of people that provide support and guidance to an individual.
Although there are formal mentorship relationships established through programs in college or in high school, the vast majority of mentor-mentee relationships happen informally, in an organic way. This is where the importance of networking comes in. Due to the lack of a professional and social network that first generation students have, it is even more imperative to develop strong networking skills. When I first learned about the idea of networking, it seemed to be regarded as a skill that people in the business field needed to have. Therefore, I did not place too much emphasis on it. These past few weeks that I have been hearing of the importance of mentorship, I have come to realize just how essential they are to one’s success. Networking skills are not optional, they are an absolute requirement. In order to catch up to more afflu ent peers who have a vast networking system and have developed good networking skills early on, first-generation students must work hard to build a network, maintain it throughout time, and build strong networking skills.
First-generation students are not the only ones with this disparity. Individuals with disabilities and mental illness also face these issues. Due to societal stigmatization and the lack of education support they face early on, they are in positions where their social network and their ability to develop strong social networking skills are greatly compromised. Therefore, they also must work hard to build a network and develop strong networking skills to open their paths to professional and educational opportunities.
Although this disparity is seen as a disadvantage, first-generation students’ experiences are meaningful in a separate way. They are experiences that cannot be overlooked because they make each person who they are. As for my experience as a high schooler and college student, while some of my peers may have been shadowing, getting guidance, and exposure to career options, I was cleaning tables at a restaurant trying to make money to support my family’s income. Even though most people would think that cleaning tables at a restaurant is a meaningless menial job, I learned so much from those early experiences working at a young age. It taught me respect for people doing these types of jobs, I developed strong work ethic, and learned to approach any task with dedication on hard work. At the same time, with my parents’ limited English proficiency, I found myself in many odd situations trying to translate for them. I not only learned responsibility and accountability, but I also learned to be an advocate for them. In this manner, I learned to advocate for myself and eventually for others. These experiences are crucial to making the person I am, and I believe the struggles first-generation students face growing up are similar and equip them with a certain set of skills and strengths.
The act of networking needs to be seen as a necessity because networking really is about self-advocacy. One idea I have learned is the importance to have the courage to be heard and be seen. As first-generation students, many times the lack of confidence in ourselves and our hesitation in letting our presence known in spaces that we have not been exposed to, keeps us from successfully building a professional network. Sometimes it is due to the belief that we do not belong in those spaces because we do not come from families with professional backgrounds. However, I have learned that to be invisible, to be silent, is a disservice not only to ourselves, but to those around us. As first-generation students, we have lived unique experiences that have shaped our thoughts and views, therefore the ideas we bring are valuable. By remaining silent in these spaces, we are robbing the world of the unique points of view that would make contributions in those spaces. Moreover, the act of self-advocacy through networking is also an act of advocacy for others. If we cannot learn to have courage to be heard and seen, we cannot learn to advocate for others who are not seen or heard. We owe it to not only ourselves and our families, but also to the underserved communities we represent.
Posted by Melinda Monge on Wednesday, December 5, 2018
By: Jasmine Richmond
When I first heard about the ChicagoCHECprogram, it sounded nice and like a good project. But all I could think of is what makes this program different from any other program that studies cancer. I thought that maybe they were testing cancer in African Americans, because I know throughout history African Americans have been used as experiments. I ended up applying and putting my heart and soul into my application hoping they felt my sincerity. No way did I think my application would be chosen, because I thought who would actually want a sick black girl to do research with. Upon receiving the news I was chosen, so many things ran through my mind, as I thought about how many other people wanted this chance. During the first week I was excited nervous and, anxious all in one, wondering about the new people I would be working with and all the new experiences I would have. During the first week I learned that there are a lot of healthcare related careers that I never knew existed.
To hear the lead cardiologist at Northwestern speak made me feel like I mattered. I never would have thought I would get to meet him unless I had a major heart problem. Dr. Yancy the lead cardiologist took time to speak to our small group which made me feel special. To hear a personal testimony from Robert Valadez , a professor from Truman College, gives me hope I can do anything. During week two I got the pleasure to meet Dr. Matthews, an incredible person doing great things in Chicago. Dr. Matthews has gotten rid of the sale of flavored cigarettes that attract children’s attention. By doing presentations in different communities Dr. Matthews has brought awareness of the cancer epidemic. During week three I have also had the pleasure of meeting Dr. Tracy Luedke. She has given me great ideas and makes me want to explore the world and give back to my community. One of my favorite presentations was Jen Cooper and how to deal with stress. It was fun, she was funny and very interactive. As I continue to work and gather information and knowledge about where I want to be, this program makes me want to be a better person. I have a group full of fun and loving people.
Working with ChicagoCHEC is one of those experiences that is hard to explain. It challenges you and make you question about all the different diseases we can control. To meet so many different people in different part of the health field I never knew existed was exciting. In school they only really teach about the basic doctors and nurses but not really about the scientists and other behind the scenes professionals. I wish more people especially the individuals in the poorer parts of Chicago could have this chance. The chance to explore, learn, and question. We need more healthcare professionals that don’t just care about the money and don’t see people as a dollar sign. I want a world where no person’s life means more than another’s. This is what I feel the ChicagoCHEC program is shining a light on –how minorities are treated in this country and other countries. Through ChicagoCHEC, I have met so many different professionals that are willing to share their stories of failures as well as successes. The professionals are always willing and happy to help us with fulfilling our dreams. Before ChicagoCHEC I have never heard of precision healthcare. Precision healthcare is specific healthcare for each individual. Knowing of healthcare made for what I need as an individual and not just what works for the majority, made me feel incredible.
During an encounter with Dr. Winn, a doctor who started precision healthcare, he said “you are not just representing yourself”. This made me think about who I represent beside myself. When I truly thought about it, I realized I represent me, my family, and all the people that look like me that came before me and that will come after me. ChicagoCHEC is doing great work within the poorer parts of Chicago, and it makes me proud to be a fellow. One of the parts I loved about the ChicagoCHEC program is the UIC Wednesday. On UIC Wednesday we gather with other groups like GUIDE and Research Start and enjoy lectures. Also during UIC Wednesday we get to go on site visits to the different locations that Northwestern and UIC work with. A lot of the different locations are small clinics in poorer areas. The people within the clinics are doing great work and are really trying to help their community.
One of my favorite site visits was to the Puerto Rican Culture Center. This center is doing great work in the community and are providing people with a great outlet. The founder of the Cultural Center is very knowledgeable and very passionate about his work. He is a proud Puerto Rican man who wants better for his Puerto Rican and black people. This site visit encouraged me to keep studying the history of my people and made when want to continue taking African American courses. Through the ChicagoCHEC program, I have found a great mentor that is a doctor in my field of study which is dentistry. This dentist took time to meet with me, so we can personally talk about how I can advance to the title of dentist. Dr Patrick Smith is one of the nicest and genuine people I have ever met. This program has made me question whether I really want to be a dentist. At the end of the day I love dentistry, when I go to sleep all I do is dream of being a dentist. This program hasmade me want to work twice as hard to become a dentist and change policies. I felt that ChicagoCHEC did a great job when it came to booking speakers that interest everyone. I am the only person that was interested in dentistry, but they made sure a dentist was there to talk to the group. There was a person interested in graphic medicine, and ChicagoCHEC managed to find someone to talk to the group about graphic medicine. ChicagoCHEC found medical students and different doctors to come speak with those of us that are interested in going to medical school. All the speakers didn’t just talk about cancer disparities, but also gave us important information on how to advance in our personal and professional lives.
During this past seven weeks we have read somegreat books. The Death Gap was one of my favorite books that we read. The Death Gap talks about how healthcare is looked at and how people are treated based on what they can they pay. This book really took a hard look at healthcare in Chicago, which is something I never really thought about. The Death Gap talks about how John Stroger as known as Cook County, Rush, and Mt. Sinai are all in the same area but only Cook County Hospital takes more of the immigrants and people of color. This was not very shocking because I personally know there are hospitals that prefer not to deal with people of color. It really just reminded me what my aunt told me when I got sick one day, “go to the white people hospital they will take better care of you there.” I know what it feels like to go to the doctor and be completely ignored and that is in no way what I want my patients to feel. Now I wonder could this be true? I believe everyone deserves the proper healthcare, no matter what race, age, or gender. As I continue on my health career path I will make sure I provide equality to all I come in contact with.
If I cannot make it as a dentist, I will go to school to get my Masters in Public Health to change policies that affect everyone. I can say I have come a long way in my thought process and I know I have a long way to go. I have been inspired by so many of my peers to be great. I will rise to the challenge and be the great dentist I know I can be. Another great book was about Henrietta Lacks. Henrietta was an African American woman whose stem cells had been used for over 20 years without her consent to develop vaccines for things like polio. This book was quite interesting because it showed how the medical system was and remains flawed. As the program comes to an end, I reflect on all the new people I have met, all that I have learned. ChicagoCHEC is doing some great work that I never knew was being done in Chicago. I previously felt like in Chicago everyone cared only about themselves, but this program has proven me wrong. Because of ChicagoCHEC I find myself helping and caring more. Like Dr. Winn said, I’m not just representing myself. I know everyone is not given this opportunity but I intend to make the best of mine.
Disclaimer
The views expressed in this paper are exclusively those of the author and not necessarily representative of the organizations the author represents nor the ChicagoCHEC organization. This work is solely intended to help further disseminate information related to ChicagoCHEC’s cause and stimulate dialogue about important topics. It is not a report by ChicagoCHEC itself and must not be treated as such.
Posted by Melinda Monge on Thursday, November 8, 2018
¡De Veras Que… Si Se Puede! It’s True That It Can Be Done
By: Queta “Ketta” Cardona
It was my 2nd semester of college at NEIU; I was in my 2nd week of class. The professor asked if anyone had applied to the summer research program at ChicagoCHEC that had been announced through email. I quickly stated, “No, it’s not for me. That’s for science people. I’m not a science person.” I was really thinking: “There’s no room for someone like me in that world. So, why even try.”
Dr. Ciecierski then talked about how any student interested in learning about health disparities and making a difference in underserved communities could apply. She also said something about how they were looking for “other” voices, too. I took that to mean that even if I did not consider myself a “science” person, maybe I could still make an impact in my community…So, I applied.
A few months later, I sat in the Baldwin Auditorium of the Lurie Research Building at the Northwestern University Campus! There I was… a door had been opened for me. And, I was being welcomed into a world of academia that I had always dreamed about, but in which I could never take part – until that 1st day of the Research Fellows Program.
Here are some insights into my experience and gains.
Aquí comparto ideas sobre mis experiencias.
Cancer – What is it?
Dr. Jonathan Moreira taught us that cancer is a spectrum of diseases; according to the NIH, cancer is the name given to a collection of related diseases. In all types of cancer, some of the body’s cells begin to divide without stopping and spread into surrounding tissues, destroying the tissue.1
Health – It is a basic right. Es un derecho.
By the end of the 1st week I learned that health care in our country is treated as a commodity. Many view it as a product that can be bought and sold, such as a loaf of bread or a car. We discussed how this approach was leaving the vulnerable, the underserved, and even us on the fringes. We studied the barriers to health care that exist in our communities: poverty, racism, education, geography, policy, etc.
And, I began to wonder about the relationship between the loaf of bread and health care. So, I asked…how can we eat if we don’t have the money for the loaf of bread? Or, what happens when we have the money for the loaf, but the store is too far away for us to buy it? How then, do we eat? How can we have health if we can’t afford to be treated? How can we be healthy if we don’t have quality care near us?
Today I understand that these barriers need to be addressed because quality health care is a basic need to which everyone should have access.
“I think my sense of what was happening to people’s health,” she explained, “was that it was really determined by what was happening in society— by the degree of poverty and inequality you had.”
HelenRodríguezTrías
El atención médica de calidad es una necesidad básica a la que todos deberían tener acceso. It’s moral and ethical.
It’s just Right! ¡Escorrecto!
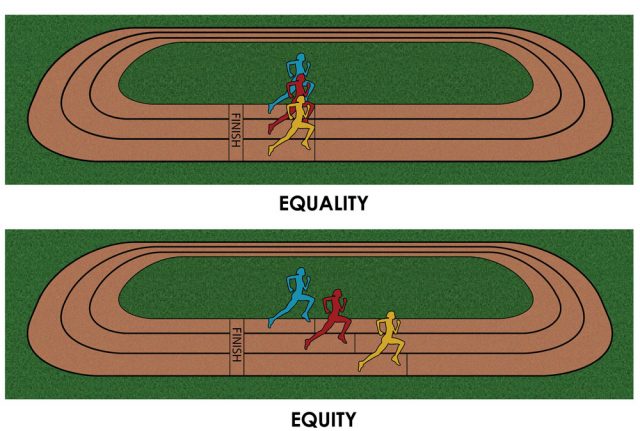
Equity – Equality isn’t always equal.
According to the (WHO), “Equity is the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically. Healthinequities therefore involve more than inequality with respect to health determinants, access to the resources needed to improve and maintain health or health outcomes. They also entail a failure to avoid or overcome inequalities that infringe on fairness and human rights norms.” 2
Journal Club was probably one of my favorite exercises in my Fellowship. We read and discussed such eye opening books as The Death Gap, by David A. Ansell and MedicalApartheid by Harriet Washington where the theme of inequity was discoursed. These discussions and other lectures helped me to grasp the difference between equality and equity. It came as a deeply personal revelation that I had never really considered how equality isn’t always equal. I am now more aware of the inequities in healthcare and strive to advocate their relief, especially in communities who have long been overlooked.
Collaborative – What we can do.
My peers were amazingly talented students from various colleges and universities in the Chicagoland area. They had varying backgrounds, career goals, and interests. Yet, we quickly became cohesive in the effort to acquire the knowledge and experience necessary to help address and change the health disparities we studied. One peer has learned to speak Spanish because she wants to make a global impact on health disparities. Another peer uses his economics degree and entrepreneurial interests to spread the message of identity and advocacy. I was also honored to work alongside a graphic designer who, after seeing the disparities in mental health treatment for the incarcerated, decided to return to get her M.D. so that she can directly serve that population.
We learned from researchers to artists. I saw that my voice makes a difference because it comes from a different yet valuable perspective. It gave me a greater appreciation for diversity in perspectives and approaches.
¿Y a hora qué?
I’m eager to return to my community and to support my neighbors as they face the issues that affect their health outcomes. I know I can personally help disseminate information on the prevention or early detection and/or treatment of cancer. I know I can direct my neighbors and friends to the community partners who offer services that help to bring health equity to my community. And finally, I will apply what I witnessed among the many guest lecturers and professors I had the honor to learn from; I will remain humble, relatable, and be part of the growing number of individuals who are closely involved with ensuring that health is everyone’s right no matter our skin color, language, neighborhood, level of education, or socioeconomic status. Sé que puedo ayudarpersonalmente a diseminar información sobre la prevención o detección temprana, y el tratamiento del cáncer.
About me:
Orgullosa de ser hija “primera generación” de padres inmigrantes mexicanos que me enseñaron el valor de mis raíces culturales. Born and raised in Chicago, I was raised by Mexican immigrant parents who gave me strong cultural and community roots. They taught me to look out for the less fortunate, which I have done for most of my adult life. After a long absence from college, I recently returned to finish my bachelor’s so that I could be better equipped to continue making an impact in the community. I plan to continue pursuing higher education with the emphasis on public health and public policy.
The views expressed in this paper are exclusively those of the author and not necessarily representative of the organizations the author represents nor the ChicagoCHEC organization. This work is solely intended to help further disseminate information related to ChicagoCHEC’s cause and stimulate dialogue about important topics. It is not a report by ChicagoCHEC itself and must not be treated as such.
Throughout my journey as a fellow in the ChicagoCHEC fellowship program, I found myself reflecting a lot on continuous cycle of constructing and deconstructing my career plan, finding ways to eliminate healthcare disparities, and learning to be an effective mentor. It was a highly informative roller coaster that put me face to face with the people involved with the healthcare system. I’ve never felt so blessed to be present at every discussion with these inspiring healthcare professionals. I learned a lot about myself, my interests on what I want to pursue, but also how we currently address healthcare disparities. I had an idea of what healthcare disparities were and how much they affected the people around me. It was a battle that seemed simple to beat that required replacing conservative politicians trying to segregate us and being part of the problem not solution. Later on, I learned that it is much more complex to fix the flaws of our healthcare system, and that some aspects may not be fixed in one lifetime. Striving for progress takes time, just like any wound. The wound in this metaphor is inequity. I approached this program with an open mind and attentive ears to see where the problems and solutions related to inequity lie while also structuring my future plans to have a better understanding of myself and the world around me.
My first week as a ChicagoCHEC fellow was quite impactful. My imposter syndrome was kicking in, I felt nervous everyday introducing myself in front of every speaker who wanted a chance to “have a brief idea who their audience was”, and seeing how my role in this group could make a difference in battling healthcare disparities. I continuously thought “why me?” a lot. I had no idea my background and race had something to do with it until we all introduced ourselves and I realized that there were no other Filipinos in the room. I’m not saying being Filipino made me better or worse, it’s just in my experience almost every Filipino I knew went into nursing. I’m also not saying that there’s anything wrong with nursing, but was there something wrong with me picking a career as a physician rather than as a nurse, based on what other Filipinos were doing? This made me wonder if I was wrong in my elevator speech to say that I wanted to be a general physician who does cancer research and that I wanted to go to the Philippines to fight for better healthcare for the poor when I felt so detached from my culture. Why did I feel so alone and different from everyone else? Everyone talked of so much passion and assurance for what they wanted to be. I felt lost, and it made me think that if I can’t help myself, then how do I get millions of people from Chicago and the Philippines to depend on me to provide better healthcare? I was also striving to find a mentor to help convince me that I wasn’t striving for something impossible. It was also during this time that my program arranged Dr. Yancy to speak to us. He said that resilience and continuing to pursue what we want in life while facing any obstacles will be very rewarding at the end when we have reached our goals. This made me aware that my self-doubt and disparities on two parts of the globe were my obstacles and that my resiliency was needed to push myself toward my goals.
I decided to take advantage of my time figuring out specifically what I wanted to do and take action instead of feeling sorry for myself. There was no better time than now to think of the various careers and fields of study that are all part of the healthcare system. I needed to stop thinking of the limits that my racial category and box of a culture that life put me in. I acknowledged it, but I wasn’t going to let it place me in a career I wasn’t satisfied with. I needed to stop the cycle in myself that hindered my self-realization. This coincided with the healthcare system in a sense. It was a continuous cycle that is so deeply rooted into our American society that it is so hard to change. Changing the mind of an individual to change the course of the outcome was simple, but changing the minds of millions of people to take action and change the outcome was so difficult.
When we met fifty high schoolers in one room, all eyes were on us to learn from and meet expectations that probably went through the roof. I had no experience with this generation of high schoolers. They grew up in the modern technological age, which was a few years after me but I couldn’t read them mentally or socially. It got to the point where I gave up over-thinking it and just spoke to them normally like I would my peers. This made me realize our same human approach to patients we don’t fully understand. We just categorize them in one group instead of individually to give healthcare at a faster and convenient rate.
In the later weeks we had some very important speakers that made me want to practice being humble more seriously as well as how I present myself. The oncologist speaker we had as well as Jen Cooper had very informative talks focusing on cancer research and the importance of networking. The importance of these presentations made me think about pursuing an MD/PhD and to basically cast a wide net to find a mentor. Learning about Dr. Moreira’s background highly resonated with my own. It was reassuring knowing that another person who has faced disparities in our medical system, limitations in family and culture, and self-doubt was able to push themselves beyond expectations and find their niche in the medical field. This was heartening to hear to make me put a little more faith in myself and what the future holds for me. His talk motivated me to learn about CAR T-cell therapy and in doing that I was able to make a decision to continue doing research either on the side while being an MD or just pursing an MD/PhD overall. At this point I felt like anything was possible. However, I was taught that without having a strategy on how to show my interest, introducing myself with an elevator speech and posture, it would be close to impossible to find a mentor willing to put time and effort advising me on my career path.
Halfway through the program things started getting more intense. I started learning more about types of cancer therapies available based on how much people can afford, a day in the life of a medical student, and a cancer survivor’s/professor’s talk that just so happened to be positioned at my own university, NEIU. I’ve never met Ben Levi until that day and he was so passionate in his talk that I couldn’t help but be fully engaged. He made me aware of more flaws in the healthcare system where our patients didn’t know the right questions to ask. That we as the healthcare providers should get off our high horse, stop spouting complex medical terminology to scared and confused patients and focus more on translating our information in a form they will understand. This talk emphasized so much on patient care and treatment, especially in the eyes of someone who has literally gone through it and continues to speak his experience. It made me realize that this practice of translational research still needs more improvement and that we as medical providers need to be active towards the change in helping the patient understand more about their disease/illness. The more patient, humble, empathetic, and honest we were towards a patient the more trust they will have in us.
Trust is the number one thing that has been emphasized during the program. It had been abused in earlier years but it can be reestablished with changes in how we approach and address patients. This experience has made me want to learn more about the African American culture, Hispanic culture, and even my own to help establish that trust into different groups to people. I now have a goal to understand, but not assume. I want to learn to communicate on an individual level, to give better patient care and to teach others the importance of this or else the gap in healthcare disparities will continue to expand. I don’t only want myself but for other healthcare providers to be that hope for their patients. The reassurance patients need that they are putting their health into the hands of someone that understands and actually cares about them as individuals. My experience here has motivated me to embrace being different, because being different doesn’t always mean that I am lost. I want to help break that cycle of unequal healthcare and be part of the change that practices patient equity every day.
ABOUT THE AUTHOR
Robynne is a senior at Northeastern Illinois University and is currently interested in pursuing medical school, conducting cancer research, as well as studying healthcare disparities.
Disclaimer
The views expressed in this paper are exclusively those of the author and not necessarily representative of the organizations the author represents nor the ChicagoCHEC organization. This work is solely intended to help further disseminate information related to ChicagoCHEC’s cause and stimulate dialogue about important topics. It is not a report by ChicagoCHEC itself and must not be treated as such.
Posted by ChicagoCHEC on Monday, September 10, 2018
Call to Action: Increasing the Number of Physicians from Underrepresented Communities as a Solution for the Need of a Culturally Competent Health Care System
By: William Mati
The physicians are the natural attorneys of the poor, and the social problems should largely be solved by them.
-Rudolf Virchow, M.D.
When my parents migrated to the Land of Opportunities, they never imagined giving birth to a child with a strong passion in changing the face of health care. Why would they? I mean, by looks of those who practiced medicine in the U.S. at the time, it seemed as if a doctor was born, not made. Fortunately, looks can be deceiving.
According to a 2018 article published by the United States Census Bureau, the population is expected to continue to diversify throughout the 21st Century1. As is the duty of a physician to meet the needs of their patient, new demands will be brought to light in a dense, multidimensional society. By equipping the health care industry with professionals from various sociocultural backgrounds, patients can be ensured that they will establish fruitful relationships with health care providers who are working to institute health equity for all.
Why is a Culturally Diverse Population of Doctors Needed Anyways? Let’s Take a Walk Down History Lane to Find Out…
Don’t worry, the entire walk is quite long. In this case, our journey is very short: 20th Century Baltimore, Maryland — where Jim Crow ideology thrived. It is here where we find Henrietta Lacks, an African- American woman commonly known among the biomedical research community as “HeLa.”2 A wife and mother of five children, Lacks passed away due to cervical cancer without ever seeing her young grow up3. On the other hand, homogenous researchers and physicians had secretly discovered a scientific gold mine after obtaining a biopsy of Lacks’ tumor, only to exploit her children years later in hopes of further developing the new immortal cell
line from their mother. In the eyes of the medical professionals assisting Henrietta Lacks, treating her (and the family) as a test subject was justified due to the “free care” given to Lacks3. Need I say, this was all done without any initial awareness or consent from the Lacks Family.
Such ethics and treatment of minority groups — particularly African-Americans — were NOT uncommon just a few decades ago. The lack of diversity among health care professionals at the time resulted in numerous voiceless communities that were simply unable to protect themselves from harmful philosophy and medical practice. As a way of pointing toward the elephant in the room, I pose the question: “How can we be the voice of the voiceless?”
Where is the U.S. Health Care System at Today?
You may have heard the relatively new buzzword among Medical Education departments across the United States: Cultural competency. By instilling an awareness and respect for the existing diversity in humanity, it is (rightly) proposed that health equity, access to health care, and the quality of care will increase for people of all sociocultural and economic backgrounds4. Indeed, this is a large step in the correct direction (recall the demographic statistics mentioned in the beginning). However, it is not sufficient.
I was fortunate to have participated in the 2018 ChicagoCHEC Research Fellows Program, a health care pipeline program that seeks to expose underrepresented students to an array of perspectives regarding cancer health disparities5. One of the primary aims of ChicagoCHEC is to ensure that the diversity of this country is reflected in the health care industry with the hopes of institutionalizing health equity for all. In fact, by doing so not only increases the likelihood of patients feeling comfortable with their health care
providers6, it simultaneously proliferates cultural competency by introducing heterogeneity directly into the Medical field. As such, patients can feel at greater ease knowing their voices will be heard — whether it is from professionals of similar backgrounds or through the courage to speak up in a place where they feel represented. By breaking down structural barriers through programs geared toward diversifying future medical professionals, the face of health care will adjust to the needs (and wants) of all patients.
I was fortunate to have participated in the 2018 ChicagoCHEC Research Fellows Program, a health care pipeline program that seeks to expose underrepresented students to an array of perspectives regarding cancer health disparities5. One of the primary aims of ChicagoCHEC is to ensure that the diversity of this country is reflected in the health care industry with the hopes of institutionalizing health equity for all. In fact, by doing so not only increases the likelihood of patients feeling comfortable with their health care
providers6, it simultaneously proliferates cultural competency by introducing heterogeneity directly into the Medical field. As such, patients can feel at greater ease knowing their voices will be heard — whether it is from professionals of similar backgrounds or through the courage to speak up in a place where they feel represented. By breaking down structural barriers through programs geared toward diversifying future medical professionals, the face of health care will adjust to the needs (and wants) of all patients.
About the Author
William Mati is a first-generation college student studying Biochemistry at Loyola University Chicago. He was part of the 2018 ChicagoCHEC Research Fellows Cohort. William plans to enroll in Medical School during 2020 with hopes of utilizing Precision Medicine as a tool for addressing Health Disparities. (Note: Any feedback or general comments are highly encouraged and should be directed to [email protected]).
Acknowledgments
I would like to thank Dr. Melissa A. Simon, M.D. and the graceful ChicagoCHEC staff, community partners, and speakers who have invested their passion and time in developing the health care professionals of tomorrow. Surely, all your work is not in vain but has planted seeds that shall flourish all across Chicago and the World.
Disclaimer
The views expressed in this paper are exclusively those of the author and not necessarily representative of the organizations the author represents nor the ChicagoCHEC organization. This work is solely intended to help further disseminate information related to ChicagoCHEC’s cause and stimulate dialogue about important topics. It is not a report by ChicagoCHEC itself and must not be treated as such.
Taylor, S. (2018). The Health Care Career Pipeline: A Program Director’s Reflection on Extending the Resources of the University to the Minority Student Community. Retrieved from https://nam.edu/the-health-care-career-pipeline-a-program-directors-reflection-on-extending-the- resources-of-the-university-to-the-minority-student-community/
Chen, F., et al. (2005). Patients’ Beliefs About Racism, Preferences for Physician Race, and Satisfaction With Care. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1466852/
“In graduate school, we are urged to publish in the most prominent journals and pursue prestigious fellowships. The number of peer citations or research dollars measures success. What is often absent is the consideration of how research affects everyday individuals. My experience with the woman at the poster session reminded me that I am not just doing research to become a known scholar in my field. I research for the sake of humanity. All researchers could use that reminder.”
Posted by ChicagoCHEC on Friday, September 29, 2017
By: Anika Jagasia
The life of a stereotypical intern can be summed up in one word – D I S O R G A N I Z E D.
When I think of the word internship, Anne Hathaway in The Devil Wears Prada immediately pops up into my head: her coffee runs, interactions between annoying co-workers, and writing hurriedly the myriad of tasks she had to do for Meryl Streep.
As the stream of anticipated worries continued to float around my mind, I plugged in the AUX and put on my go-to playlist. Spotify’s Good Vibes.
“Ma’am, do you need help, are you lost?”
I had to explain to the lady at the front desk that it was V I T A L that I not be late for my first day of my internship at Northwestern University’s Simon Laboratory where I would be assisting the Simon team.
After a mixed look of pity and sympathy, I stepped in the elevator and exited onto the 18th floor in front of two very heavy double doors. I grabbed one of the door handles, pushed it open, and was quite startled as both came apart with an unleashing amount of force, leading me to stumble back in surprise.
Five minutes later I was testing out how far back I could lean in my foamy office chair. Across from me sat my new cheery supervisor, Jen. While she explained the role of the Simon team–to promote health and healthcare equity for culturally diverse and underserved communities–she rattled off a few words I wasn’t familiar with. Uh oh. Inequities, Disparities, and Equity vs. Equality. After receiving a patient and thorough explanation I realized that some high schoolers like me don’t know these terms or the problems they entail.
…. Here is where my personal story ends and my post begins ….
The Knowledge Gaps
I want to share some major problems that are in healthcare and what I’ve learned from them during my time in the Simon Lab this summer. By the time you finish reading this article, you will enter the loop of knowing the health dilemmas at hand, know how to continue spreading awareness through educating others, and even be exposed to opportunities through which you may pursue your interest in promoting healthcare equity. Here are the basics that I will cover: health inequities, disparities, and equity.
The first thing to know in promoting health equity is…you guessed it…equity.
Some people may assume that equity is the same thing as equality. However, surprisingly, there’s quite a large difference. You and your friends are at a track, lined up and ready to race each other. You’re all pumped up and ready to go, but you look over and realize your friend Blue–on the inner lane–has the biggest chance of winning since they have the shortest distance to run. Everyone starting at the same starting line was equal–but equality did not yield a fair race. To be equitable would have been to accommodate everyone’s position on the track so that they would run the same distance. So, to make the race fair Person Blue, Red, and Yellow would start at different points on the track to run the same distance. This is the difference between equality and equity. To be equal is giving everyone the same resources without regards to what they need or where they are starting from. To be equitable is to give everyone resources that take into consideration their individual needs and providing resources to them accordingly.
Now, going back to my first meeting with Jen, I will introduce you to a main focus in the Simon Lab – Health Disparities. Even though my knowledge was a bit too simplified to totally understand everything that Jen was saying, I grasped the fact that cancer disparities are a HUGE problem, especially in Chicago. For a moment, with all the new lingo I felt like I was living in A Devil Wears Prada Moment. I [Anne Hathaway] was standing in front of Jen [Meryl Streep] who was saying all this important information, but I was struggling to write it all down, eventually, giving up because there was too much to write.
Before we get into the projects that I would be doing relating to cancer disparities, I first had to understand what a health disparity is in general. I will admit that it took a few days of being immersed in my internship and working on cancer disparity projects to grasp what health and cancer disparities are.
Simply, a health disparity is a condition where there is a higher risk for Group A compared to Group B. I learned that it used to be believed, and sometimes still is, that it was biological or had to do with genetics. Unfortunately, the problem is more complicated than that in most cases. There are a myriad of factors that negatively affect groups of people: socioeconomic status, gender, age, disability, geographic location, and more.
It wasn’t until about 1980 that statistics showed that the average life expectancy for the US had grown by 25% to 75 years. While life expectancy was improving, minority groups faced shorter life expectancy, higher rates of cancer, diabetes, strokes, substance abuse, infant mortality, and lower birth weights. (To see some Cancer Disparities-specific statistics see the bottom of this post!)
A Call to Action to Improve Health Inequities – An Argument for Education
We need education. Truthfully, I was surprised to see how the issue of health disparities is so pressing, and – in high schools … my high school – it is not a common subject or element of most curriculum. But, we can’t blame our schools. I haven’t been exposed to many articles in the news talking about health disparities, or seen segments about it on TV, or read about it in magazines/newspapers. Is there enough current news on health disparities out there? Should we put out more articles on the topic to spread awareness? Regardless, we can do more to educate, especially the younger generation. Educating future generations about our battle with cancer disparities is one of the most effective methods we can use to put our foot down on these inequities. We need to offer opportunities to learn about persisting issues, which will inevitably be training our future generations how to tackle healthcare problems. Students as young as middle school need to learn about the persisting issue, so the future for cancer disparities doesn’t have to look so grim. As a result from the education and training individuals will receive, the level of community engagement will increase, and awareness will spread.
We – students – need to be engaged in our education and our careers. When I found the organization called CURE — an organization within the National Institutes of Health — I was wowed by how they took the future in improving cancer disparities to a new level. CURE’s mission, like many others, is to offer career development opportunities to strengthen and diversify the field of cancer disparities. The unique part of the organization is that students as young as middle school, high school, and even undergraduate students can work alongside scientists. How cool is that? This is where we see the step 2 and 3 involved–training and community engagement–and CURE incorporates all 3 Not only do they engage a community, but include the whole nation! CURE understands that training the future generations is important and they are spreading awareness by offering these amazing opportunities for kids. Students can even have a mentor scientist or researcher!
We need more organizations to follow in ChicagoCHEC’s footsteps to help advocate for healthcare as a whole. Without organizations like ChicagoCHEC, health inequities would remain an issue, and perhaps proliferate into chaos.
So, what do you say, will you join in changing the future of cancer disparities?
Anika Jagasia is a rising Senior at Latin School of Chicago. She worked in Dr. Melissa Simon’s Lab at Northwestern University – a lab focused on health inequities and social issues for underserved, low-income individuals – for the summer. Anika plans to attend college in the Summer 2018, with an interest in the Sciences. Her opinions are her own and do not reflect the views of Latin School of Chicago, Northwestern University, or ChicagoCHEC. Check out Skinny Trees Podcast: An Exploration of Health Inequities in & around Chicago in for an interview conducted by Anika with Dr. Joe Feinglass, a health services researcher, Professor, and long standing social activist.
A Healthier Back of the Yards: Increasing Services to Decrease Violence
By: Angel A. Jimenez
Shootings, death, and drugs: this is how Back of the Yards is portrayed in the media. There is a widely shared opinion that my community does not want to be helped, does not want to change, and is always looking for trouble. The Back of the Yards community is located in the south side of Chicago, which was once home to the Chicago Union Stockyards, most notably known because of The Jungle, by Upton Sinclair. Back of the Yards was home to Germans, Irish, and Czechs in the 1870s. Later, Poles, Lithuanians, and Slovaks would become the majority. Small numbers of Mexican immigrants arrived during the 1920s and World War 1. By the 1970s, when the Union Stockyards were closed, the community was primarily Mexican with a minority of African Americans. Today the Back of the Yards suffers from economic decline, social inequality, poor housing, and poor working conditions in nearby factories.
In a recent study conducted by the Brighton Park Neighborhood Council, 369 people from my community were asked three questions: What are some mental health concerns you have? What are some barriers that are faced? Would you consider receiving emotional support? In this survey, it was found that some of the most prevalent concerns are depression, anxiety, isolation, and trauma. Furthermore, some barriers that were mentioned are the cost of health services, lack of insurance, language, stigma, and the lack of accessible services. Finally, 80% of those who were surveyed said that they would consider receiving emotional support if it was available in the community. I believe this survey shows that my community wants help, is not looking for trouble, and wants change to happen.
It is very easy to point fingers and blame the violence in my community on the people that live there, however we – the residents of Back of the Yards – would like some answers. I noticed that several helpful community resources have recently been closed. Why was the mental health clinic closed? Why was the Healthcare Alternative Systems (HAS) organization’s office, which provided help to victims of domestic violence, anger management services, youth outreach, and many other services needed in the community, closed? Why do schools have to look for grants in order to better help the children in my community who suffer from various mental and emotional stresses? We ask for support and oftentimes are ignored and told that more police will help reduce the violence in the community because that is the biggest problem. The violence in the community does affect us and the trauma affects every part of our lives, but we also aren’t able to provide the appropriate support to help people deal with grief, anxiety, fear, and depression, among other mental health issues. In my opinion, that is the biggest problem in the Back of the Yards.
Fear and anxiety can make us do things that we cannot understand. Mental health institutions and organizations like HAS exist to help people learn how to cope with their fears and manage anger and stress. Recently, the Donald Trump administration’s immigration policies have incited a newfound level of anxiety and fear in the community. Not to mention, in the beginning months of this year, the Immigration and Customs Enforcement (ICE) agents were present in the neighborhood. People were afraid to leave their homes and did not feel comfortable participating in routine, everyday activities such as grocery shopping.
Mental health is not being properly addressed in the community and the effects are plaguing its residents, mostly youth. Around 34% of residents in the Back of the Yards are below the age of 19. An article I read for my biology class explained how poor mental health in children can be especially toxic. It can hinder their brain development and can also hinder their academic success in school. Sometimes children find themselves lost, not knowing where to go. As a result, they decide to find a new family on the streets. Children live out the stress and anxieties of their parents and they do not know how to work through and process everyday stressors.
Call to Action: Creating a More Positive and Healthy Future
If our aldermen would provide funding for programs in schools and churches and create or re-open more programs focused on mental health, like HAS, we could provide a safe and nurturing environment for parents and children. More programs that are aimed at youth will help them transition from childhood to adulthood in an environment void of depression, anxiety, or grief. This will also equip our youth with the skills necessary to identify their feelings and develop a toolbox of strategies that they can use to help themselves and others. Then, when our youth get older, they can continue helping the generations that follow. There are already some existing programs in the neighborhood that are trying to help teens, but they are not able to help everyone. They require more funding, people, and space to be able to reach more families.
Before judging Back of the Yards solely on what is shown on television, I invite you to come visit us. Learn about our struggles, our fears, and sorrows, but also learn about the programs and people already making a difference in our community. Help us by committing time to our neighborhood. Bring workshops on mental health, share information with schools and institutions in the community, or help us develop and fund programs for our youth and families. Back of the Yards should not be known for its shootings and violence, it should be known for its resilience and its work towards creating a more positive and healthy future.
For more information about the Back of the Yards, please visit the Back of the Yards Neighborhood Council website: http://www.bync.org/
About Me
My name is Angel Jimenez. I am currently a sophomore at Whitney Young Magnet High School. I am a member of the Holy Cross/IHM Marimba Ensemble which is a group for youth from the Back of the Yards community, who are interested in music. The program was created in the early 90s to bring youth together through music. Each generation of marimba players learns music by ear and are taught by former marimba players. We volunteer our time and play at various events in the Chicagoland area. I am also entering my second year in UIC’s Medicina Academy Apprentice Program which guides and supports high school students in pursuing a career in medicine through seminars about college, medicine, inter/intrapersonal activities, and career opportunities in the healthcare field. I am interested in becoming a physician and possibly applying my love for music by exploring a career in music therapy and medical research.
Join ChicagoCHEC and the UI Health Cancer Center at one of Chicago’s largest Back-to-School events – providing FREE Back packs and school supplies, immunizations and physicals (bring records), Social Service information around employment, education, insurance, immigration and housing, Hair-cuts and a BLOCK PARTY KidZone with bouncy houses, carnival games, candy, music and FUN!
May 3rd – May 5th, 2017 Northeastern Illinois University
Chicago, IL USA
Deadline for Abstracts is Friday, March 17th, 2017
Faculty/Researcher Abstracts for Oral Presentations must be submitted to:
Elena Navas-Nacher, PhD, MS [email protected]
Students Abstracts for Poster Presentations:
Emma Turian, PhD [email protected]
Continuing in the spirit of six earlier meetings organized by the ISI Committee on Risk Analysis (ISI-CRA) of the International Statistical Institute, this year’s conference focuses on Cancer-Related Risk Analysis.
The format for the meeting will include plenary talks, organized sessions, and sessions with contributed talks and posters. The conference includes keynote presentations by world-renowned scientists. Students are encouraged to enter a poster competition and present their projects to conference attendees. There are no events scheduled simultaneously so you will not miss anything. A Gala Dinner will be held on Thursday, May 4th and will feature a keynote presentation, a student poster award ceremony and live entertainment.
The ICRA7 will be followed by NEIU’s 10th Workshop on Mathematical and Statistical Modeling, which will begin at 1:00PM on Friday, May 5th, 2017 and continues through Saturday, May 6th, 2017 at Northeastern Illinois University’s Main Campus. For general conference information please email[email protected].
To learn more about the event, please visit the website.
Join us for a special event with leading experts to help you learn about your risks, why screening matters and how to take important steps toward prevention.
WHEN:
Wednesday, March 15th
1:00-3:30 p.m.
WHERE:
ACCESS Center for
Discovery and Learning
5139 S. Ashland Ave.
Chicago, IL 60609
RSVP to Shawn Foster
at 773.247.2435
or via email at [email protected]
Posted by ChicagoCHEC on Thursday, December 15, 2016
Events, Funding Opportunities, Calls for Paper and other Resources are all your fingertips in the monthly bulletin provided by the Alliance for Research in Chicagoland Communities (arcc), a program from Northwestern University’s Center for Community Health.
Posted by ChicagoCHEC on Tuesday, December 6, 2016
We are excited to announce that the ChicagoCHEC Research Fellows program is now accepting applications! This program is geared toward first-generation and underrepresented minority students interested in health or research careers. Apply soon – deadline for applications is February 15, 2017.
About the ChicagoCHEC Research Fellows Program
The ChicagoCHEC Research Fellows Program is a comprehensive learning experience for undergraduate and postbaccalaureate students at Northeastern Illinois University, University of Illinois at Chicago, Northwestern University, City Colleges of Chicago, and other Community/ Junior Colleges in the Chicago metropolitan area. We are seeking outstanding undergraduate and postbaccalaureate students with an interest in health and health care who possess the commitment to apply to graduate or medical school and can bring diverse perspectives and experiences to advance the nation’s work toward cancer health equity. ChicagoCHEC Research Fellows will spend the summer in seminars and research rotations learning from leading scientists. Following the summer intensive program, ChicagoCHEC Research Fellows will have the option to be matched with a research mentor and research project during the academic year.
Application Deadline: February 15, 2017
Program Dates
June 19 – August 11, 2018: summer intensive experience
Fall 2017: optional research team placement
Want to learn more about health equities in your city? Do you enjoy podcasts? Check out Skinny Trees, a podcast born out of ChicagoCHEC that aims to continue the conversation about health equities in and around Chicago.
To learn more, check out www.skinnytreespodcast.com. Episode 1 features Dr. Melissa Simon, ChicagoCHEC Northwestern University Principal Investigator, discussing how to decipher the nuances of health equity language.
Posted by ChicagoCHEC on Friday, September 30, 2016
We are excited to announce that our ChicagoCHEC Incubator and Catalyst Funding Program’s 2016-2017 Request for Proposals is now open. One of the most important needs for growing an idea is early stage funding. Do you need seed funds to take your cancer disparities project to the next step? The ChicagoCHEC Research Incubator / Catalyst Funding Program supports transdisciplinary cancer disparities research in behavioral and social science, basic, biomedical, and translational science. These awards are intended to foster cross-institutional collaborations among investigator teams from NEIU, UIC, Northwestern, and community partner(s). ChicagoCHEC funding opportunities consist of:
Partnership Development Incubator Grants: 1 year seed funding of up to $40,000 to jumpstart partnerships to develop research across the three institutions and with community partners.
Proposal Development Incubator Grants: 1 year seed funding of up to $40,000 to help teams progress from partnership phase to proposal writing phase.
Pilot Project Catalyst Grants: awards of up to $120,000 per year for 2 years across the three institutions and community partner(s).
This is a unique funding opportunity that requires involvement from all three institutions (NEIU, UIC, Northwestern) and a community stakeholder. ChicagoCHEC offers help linking interested people with potential collaborators across institutions and communities.
A pre-proposal consultation meeting with ChicagoCHEC is due December 15, 2016 and applications are due January 15, 2017. For more information please see the Request for Proposals or email [email protected].
The ChicagoCHEC Catalyst & Incubator Grant Program is pleased to announce the 2016 grant recipients. All investigative teams have proposed novel approaches to addressing cancer disparities and are devoted to advancing cancer health equity through cross-collaboration, high-quality research and unwavering dedication to training and education. It is anticipated that all projects supported by the ChicagoCHEC Catalyst & Incubator Grant Program expand to become larger, long-term grants such as R01s.
Project 1 (Partnership Development Grant):
Reducing Colorectal Cancer Disparities on the South Side of Chicago through Cross-Institutional Collaboration
Principle Investigators: Danielle Lazar, AM, DrPH Candidate (Access Community Health Network), Kenzie Cameron, PhD (Robert H. Lurie Comprehensive Cancer Center of Northwestern University), Hardik Marfatia, PhD (Northeastern Illinois University), Shan Wang, PhD (Northeastern Illinois University), Kameron Matthews, MD, JD (University of Illinois Chicago), Karriem Watson, DHSc (University of Illinois Chicago)
Project 2 (Proposal Development Grant):
Community-Engaged Obesity Intervention Development for Puerto Rican and Mexican Men
Principle Investigators: Lisa Sanchez-Johnsen, PhD (University of Illinois Chicago), Magdalena Nava, BA (Puerto Rican Cultural Center), Leonilda Calderon, BA (Puerto Rican Cultural Center), Amanda Dykema-Engblade, PhD (Northeastern Illinois University), Alfred Rademaker, PhD (Lurie Cancer Center)
Project 3 (Pilot Project Catalyst Grant):
Prostate Cancer Disparity in Chicago-Area African American Men: Patient-derived Models and Biomarkers of Cancer Risk
Principle Investigators: Larisa Nonn, PhD (University of Illinois Chicago), Sarki Abdulkadir, MD, PhD (Lurie Cancer Center), Cindy Voisine, PhD (Northeastern Illinois University), Adam Murphy, MD (Lurie Cancer Center / Jesse Brown VA), Marcus Murray, BA (Project Brotherhood)
The Chicago Cancer Health Equity Collaborative (ChicagoCHEC) is a National Cancer Institute comprehensive cancer partnership led by the Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Northeastern Illinois University, and the University of Illinois at Chicago. Our mission is to advance cancer health equity through meaningful scientific discovery, education, training, and community engagement.
On June 20, 2016, the Chicago Cancer Health Equity Collaborative (ChicagoCHEC) kicked off their inaugural Summer Research Fellows Program — a comprehensive, paid eight-week summer learning experience for undergraduate and post-baccalaureate students from Northeastern Illinois University, Northwestern University, University of Illinois at Chicago (UIC), and the City Colleges of Chicago (CCC).
Focused on developing academic, technical, and professional skills, the Fellows Program will help prepare a new generation of leaders for careers in social, behavioral and biomedical research, and in healthcare. ChicagoChec Research Fellows will gain important knowledge, skills and networks through immersion experiences, group projects and journal clubs. In addition, one-on-one, group, and near-peer mentoring will guide their progress in becoming researchers and healthcare professionals who can bring diverse perspectives and experiences to advance the nation’s work toward cancer health equity. At the conclusion of the program, Fellows will have learned fundamental research practices and methodologies, pertinent research content topics (e.g. cancer inequity and recruitment of underserved minorities in clinical trials), social contexts for health inequity across the cancer continuum, and critical professional development practices and networks.
The Summer Research Fellows Program leverages the expertise of the scholars, cancer researchers, health professionals, and institutional and community leaders who participate as guest lecturers, project mentors, and site visit hosts. According to the physician-scientists and researchers who lead ChicagoCHEC — Northwestern University’s Melissa Simon, MD, MPH, UIC’s Robert Winn, MD, and Northeastern Illinois University’s Christina Ciecierski, PhD, and Moira Stuart, PhD — the program provides an opportunity to do things differently than they’ve been done in the past. That is, to move the needle on health equity by expanding opportunities to the next generation in a way that changes the architecture of collaboration, community engagement, and the culture of research education.
“The Summer Research Fellows program is a first-of-its-kind program to advance research, leadership, and community-engagement capabilities in this high-potential group of first-generation, underrepresented minority and non-traditional college students,” said Simon, the George H. Gardner, MD, Professor of Clinical Gynecology in the Department of Obstetrics and Gynecology at Northwestern University Feinberg School of Medicine and Co-Leader of the Lurie Cancer Center’s Cancer Control and Survivorship Program. “The interest in ChicagoCHEC’s first program was so great that we were inspired to create an Affiliates Program as a pipeline for participants in the future.”
Funding support for ChicagoCHEC is provided by the National Cancer Institute (grants U54CA202995, U54CA202997, and U54CA203000).
About ChicagoCHEC
The Chicago Cancer Health Equity Collaborative (ChicagoCHEC) is a National Cancer Institute comprehensive cancer partnership led by the Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Northeastern Illinois University, and the University of Illinois at Chicago. Our mission of ChicagoCHEC is to advance cancer health equity through meaningful scientific discovery, education, training, and community engagement.
We have some exciting undergraduate cancer research internship opportunities planned for this summer! The program is geared toward first-generation and underrepresented minority students interested in health or research careers. Apply soon – deadline for applications is February 29, 2016.
About the ChicagoCHEC Research Fellows Program
The ChicagoCHEC Research Fellows Program is a comprehensive learning experience for undergraduate and postbaccalaureate students at Northeastern Illinois University, University of Illinois at Chicago, Northwestern University, and City Colleges of Chicago. We are seeking outstanding undergraduate and postbaccalaureate students with an interest in health and health care who possess the commitment to apply to graduate or medical school and can bring diverse perspectives and experiences to advance the nation’s work toward cancer health equity. ChicagoCHEC Research Fellows will spend the summer in seminars and research rotations learning from leading scientists. Following the summer intensive program, ChicagoCHEC Research Fellows will have the option to be matched with a research mentor and research project during the academic year.
Application Deadline: February 29, 2016
Program Dates
June 20 – August 12, 2016: summer intensive experience
Fall 2016: optional research team placement
Since our official launch in October of 2015, ChicagoCHEC has been a buzz of activity, as we launched out the gate to transform our many ideas into reality. We are excited to have this incredible opportunity to move the needle on health equity, and we want all of you at the table. Keep an eye out in this space as we continue to roll out new programs, opportunities, resources, and ways to engage. (we only ask that you bear with us as we grow!)
Welcome to the Chicago Cancer Health Equity Collaborative (ChicagoCHEC) blog! What is ChicagoCHEC, you might ask, and why are we blogging?
ChicagoCHEC is a comprehensive cancer partnership led by Lurie Cancer Center of Northwestern University, the University of Illinois at Chicago, and Northeastern Illinois University. Our mission is to advance cancer health equity. We strive to do so by way of meaningful scientific discovery, education, training, and community engagement.
Advances in cancer health equity take creativity, out of the box ideas, active community voices, and an open exchange of ideas and practices.
We intend for this blog to support the work of the ChicagoCHEC community and to create a safe space for everyone to share ideas. We hope this blog will stimulate new thinking and lively discussions as we share our ongoing work toward cancer health equity. Whether you’re a faculty member, student, staff, or community member, we welcome you to join this dynamic learning space.
What can you expect to see here?
ChicagoCHEC faculty, staff, students, guest bloggers and other creative thinkers commenting on the latest scientific and healthcare advances, their projects, activities, and anything under the sun
Events announcements
Information about resources
Research, training, and community engagement opportunities
Our doors are wide open to ideas. We want this blog to foster interactions with a broad community of thinkers and doers. We invite you to contribute your ideas to help make this blog timely, lively, and a place where we can all learn together. Ready, set, go!


 Why is a Culturally Diverse Population of Doctors Needed Anyways? Let’s Take a Walk Down History Lane to Find Out…
Why is a Culturally Diverse Population of Doctors Needed Anyways? Let’s Take a Walk Down History Lane to Find Out…